




Headache and neck pain often intersect, with nerve compression potentially being the underlying cause. A team of researchers led by Dr. Pamela Blake and Dr. Rami Burstein is investigating the potential of a surgical approach to address this issue. In this article, we delve into their groundbreaking research, explore how nerve compression might be impacting your symptoms, and examine the potential for surgical solutions to provide relief. Discover the latest insights and what they could mean for treating headache and neck pain.
Patient Story: My Neck is Killing Me
For the last few years, my neck has been killing me. I’ve had migraine attacks since I was 15, but they were occasional. Slowly, things deteriorated. I sit all day at work and stopped exercising a few years ago. My posture isn’t good. The chiropractor helps for a while, but the pain always comes back. I can’t do anything with my arms in the air for too long. Sometimes, there’s pressure in my neck that goes to my shoulders, followed by a full-blown migraine. Is this my life? Can’t I just be fixed somehow?
Why would a neck problem cause a migraine attack?
The nerves of the neck and head all connect in the same place in the brain. Two zones that are especially linked are the forehead/temples (V1) and the occiput and upper neck (C2-C3). Anatomically, the head and neck are part of the same pain zone. This link is bidirectional: a neck problem can cause a migraine attack, and migraine can induce neck pain.
I heard that migraine was a disease of the brain, where does the neck fit in?
Migraine is a disease of the brain. We know that the migraine brain has unique chemical and electrical characteristics and that many genes contribute to this special “software.” This is the “central” theory of migraine, where the key culprits are the brain networks. However, the brain is always reacting to the environment, and pain signals can trigger the migraine cascade. The neck is a site of pain directly connected to the brainstem zones responsible for headache. It’s not surprising, then, that neck pain could trigger migraine attacks.
What prompted the researchers to study this topic of neck and headache?
Patient stories and symptom descriptions were key. Both Dr. Blake and Dr. Burstein noted that:
- Many patients with migraine also complain of neck pain.
- These patients did not show much improvement with medications targeting the brain.
- Interventions targeting the neck, such as manipulations, blocks, and even surgeries, were sometimes effective.
It’s important to be cautious about the effectiveness of surgeries due to the high placebo effect associated with them. Nevertheless, the idea that targeting the neck could help some patients couldn’t be entirely dismissed.
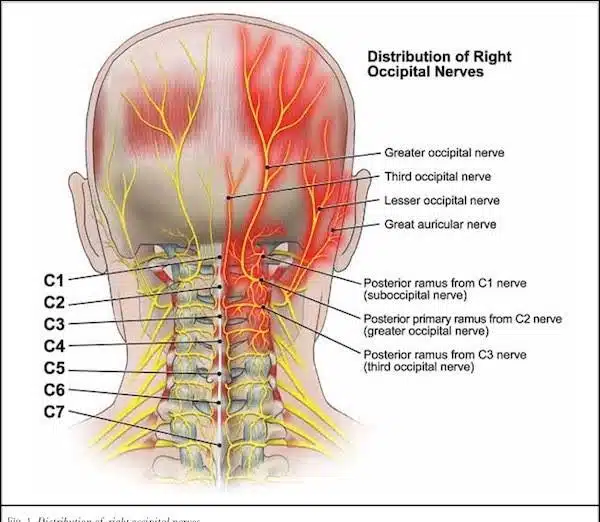
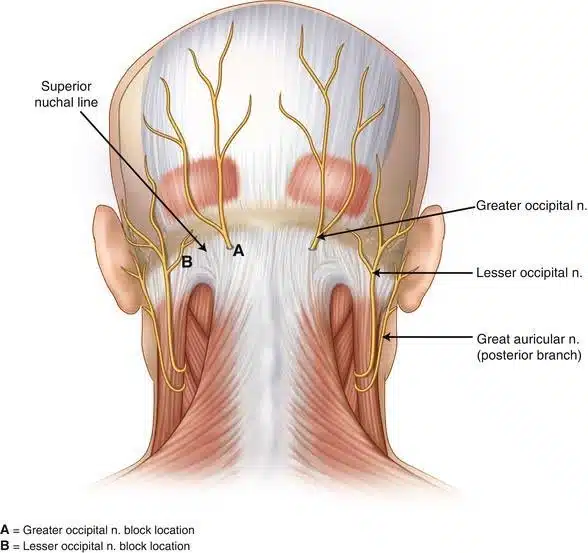
What could cause a compression of the occipital nerves?
The occipital nerves (greater and lesser) pass through different layers of muscle before reaching the skin of the occiput. Anatomical and surgical studies have identified multiple potential compression sites along this path. Unfortunately, we do not yet have imaging techniques to visualize these compressions. Even MRI cannot demonstrate them.
What did the researchers do to prove their theory?
Dr. Burstein, Dr. Blake, and their teams embarked on a true scientific journey. Studies were conducted on animals and then humans to better understand the anatomy of the neck nerve fibres. They demonstrated that some nerve fibres for the neck cross the skull to go inside and connect to the meninges and observed signs of compression of these nerves during surgery. They also found signs of inflammation in the nerves of people with chronic migraine. We can compare this to sciatica, where a compressed nerve root leads to pain in the leg and lumbar spine.
The researchers proposed that inflammation of the neck nerves could lead to inflammation inside the back of the head, causing chronic headaches. In individuals with migraine, this inflammation could trigger more attacks and lead to chronification. This would be an example of the “peripheral theory of migraine.”
Should we consider surgery (decompression of the occipital nerves) to treat migraine?
The researchers published seven patient stories after surgery. Some patients improved significantly, while others did not. The current challenge lies in predicting who could genuinely benefit from surgery and identifying the most appropriate surgical approach. The difficulty is compounded by the lack of effective imaging techniques to visualize cervical nerve anatomy. Additionally, symptoms vary, and people express them in different ways. The physical examination of the neck is also complex, as it’s difficult to pinpoint the exact source of pain just by pushing on the occiput. The question of placebo must also be addressed, as physicians should not expose people to surgeries that are not truly effective.
What’s the conclusion? Should I look for a surgery?
The issue of neck pain linked with headache and migraine is significant, as many patients are disabled by these symptoms. Any doctor treating migraine patients and willing to listen understands this. However, science is based on observations and facts, not just symptoms and hypotheses. It is too early to recommend whether decompressive surgeries should be used, and ongoing research is necessary. This therapeutic option could become officially recognized after sufficient testing.
References
- Blake P, Burstein R. Emerging evidence of occipital nerve compression in unremitting head and neck pain. J Headache Pain. 2019;20(1):76.
- Blake P, Nir RR, Perry CJ, Burstein R. Tracking patients with chronic occipital headache after occipital nerve decompression surgery: A case series. Cephalalgia. 2019;39(4):556-563.
Post #3031

