



Preventive Treatments
Preventive treatments for migraine aim to reduce the frequency, severity, and duration of migraine attacks. Unlike acute treatments, which are taken during a migraine attack to help relieve symptoms, preventive treatments work in combination with lifestyle adaptations to prevent or lessen the intensity of an attack.
On this page, you will find:
List of Migraine Preventives Available in Canada
(Classes, Mechanism of Action, Side Effects)
Common Questions About Starting and Using Preventive Medications
Migraine Canada Videos, Articles & Resources about Preventives
Table of Migraine Preventives: Classes, Mechanisms of Action, and Side Effects (see our Preventive Dosing Guide)
Additionally, here is the table of therapies with no strong evidence of efficacy (more research needed OR strong placebo effect suspected):
Frequently Asked Questions
How do I know if I need preventive medication?
There is no absolute rule. The impact of migraine on your life is the main factor. Generally, when people have 4 or more migraine attacks per month, the impact is significant enough to consider prevention. Still, making changes to your lifestyle can be a first option. If you are having more than 10 days of migraine attacks per month, the risk of becoming chronic is very high and a preventive should be prescribed. Anybody with chronic migraine (>15 days per month) should try preventives.
Will my healthcare professional decide if I should take a preventive medication?
The decision to take preventive treatment is yours. Discuss the pros and cons with your physician or nurse practitioner. Establishing clear expectations of your treatment goals and having a plan you’re comfortable with is key.
What is the effect of preventive medications on my brain? How do they decrease migraine attacks?
There are several types of preventive medications and they act through different mechanisms in the brain to increase the migraine threshold (the limit your brain has for migraine occurrence) and make the brain less susceptible to triggers that result in a migraine attack.
Why was I prescribed a drug for depression/blood pressure but I am not depressed/my blood pressure is normal?
Older migraine preventives have not been designed specifically for migraine. Often, their effect on migraine has been observed by people who were taking them for other reasons. Remember that medications may have different effects on the brain and body. For example, blood pressure drugs also have effects on brain networks. You are not being prescribed these medications because your healthcare professional thinks that depression or blood pressure are the cause of your migraine.
Are preventive medications dangerous?
Like any medication, preventive medications have possible side effects and risks. Some people should not take some of these medications for medical reasons, it is up to your doctor or nurse practitioner to check which treatment is best for you.
How will I know if my preventive medication works?
Track your baseline migraine frequency with a headache diary! Improvement can be seen in reduced frequency and severity of attacks, better response to acute treatments, and overall quality of life.
What can I expect as a benefit?
Ultimately, the goal is to decrease the impact of migraine on your life. There are two types of improvement: on frequency and on severity.
- A preventive treatment decreases migraine frequency by 50% in 50% of patients who try it. Some people may have a “super response” to some medications (75% better).
- Severity can also decrease: you may have less nausea, your acute treatments may work better, you may be able to miss work or activities less often. Often if migraine frequency remains the same, but the severity decreases, this is enough reason to continue the preventive treatment.
Other signs of improvement can include:
- Less sensitivity to triggers
- Better effect of acute medications
- More ability to plan activities
- Better mood and sleep
What is the best migraine preventive?
There is no one-size-fits-all solution. People with migraine have different brains and different bodies. At the present time, no one can predict who will improve with a certain medication or not. Trying different options is key.
According to the CHS, here is an approach to finding the right preventive drug:
- First time using preventive medication, start with a blood pressure lowering medications - Propranolol, Nadolol or Metoprolol OR an antidepressant - Amitriptyline
- If people desire low side effects: blood pressure medication - Candesartan or Lisinopril OR herbs/vitamins - Magnesium, Riboflavin or Co-enzyme Q10
- People who are overweight: Topiramate
- People with high blood pressure: Propranolol, Nadolol, Metoprolol, Candesartan or Lisinopril
- People with depression/anxiety: Antidepressants - Amitriptyline, Nortriptyline or Venlafaxine. People with depression should not take flunarizine
- People with migraine not well controlled on 1 medication alone: combination therapy with 2 different drugs
- Migraine during pregnancy: avoid drugs if possible. If not, consider - Magnesium, Propranolol, Metoprolol, Amitriptyline or Nortriptyline. Please note, Valproic acid and Topiramate should be avoided in pregnancy due to the known risks associated with the fetus.
- Migraine during breast-feeding: avoid drugs if possible. If not, consider - Magnesium, Propranolol, Nadolol, Metoprolol, Amitriptyline, or Nortriptyline.
- People with seizures: try one of the migraine prophylactics that are also anti-seizure drugs.
- People with asthma: avoid beta-blockers
What side effects can I expect?
Side effects vary by medication and are often mild and temporary. Not everyone will experience side effects. If the effects are mild, like dry mouth or minimal sedation, and your migraine has improved, it may be worthwhile staying on the medication. In consultation with your doctor, it is a personal decision to weigh the pros and cons.
It is important to note that side effects often occur quickly but it may take longer to see a benefit from the preventive medication.
What are the doses, side effects, and contraindications of migraine preventive medications?
They differ depending on the medication. For more information, please see our post on doses, side effects, and contradictions.
Will the medication make me gain weight?
Some preventives are associated with weight gain, others with weight loss, and many are weight neutral. If you do start a preventive that can cause weight gain, monitor your weight and diet.
How long do I have to try the medication?
Preventive medications need to be taken at effective doses for several months. One month is never enough to make a decision.
- For oral preventives (excluding gepants), it usually takes a month to titrate up on the dose and 2-3 months on the effective dose to see full benefit.
- For Botox, at least 2 cycles (3 months apart) is recommended.
- For CGRP antibodies, a trial period can be between 3 and 6 months (even though some people improve right away).
Migraine attacks often occur in cycles, with periods of increased frequency followed by times of relative calm. Various factors, such as less sleep, more stress, new medications, or hormonal changes, can trigger these episodes, but sometimes the reasons are unclear. If your migraine frequency rises, do not stop your preventive medication, assuming it has lost its effectiveness, as this can worsen your condition. Instead, keep a diary to identify potential triggers or aggravating factors. It's a common mistake for people with migraine to stop their preventive treatment out of frustration, especially during difficult periods. If the increased frequency persists for many weeks, consult your physician, as it may be more effective to adjust your dosage rather than discontinuing it.
If I start a preventive, will I have to take it all my life?
Preventive agents are not necessarily used for many years. After 8-12 months of successful treatment, one could slowly taper and try to discontinue the preventive medication. If migraine attacks increase, then the treatment is still needed and may be continued.
Long term treatment may be required for some people. Research shows that continuing with a preventive increases the chances of remaining stable in the long term. If something works, keep doing it!
Will I become addicted to my preventive medication? Should I stop taking it?
Preventive medications do not cause addiction (opioids and cannabinoids do). If effective, they are continued for at least a year before considering a dose reduction. Always consult your healthcare provider before stopping any medication. If you decide to taper down, do it very slowly. Never stop preventive medications abruptly, as this could trigger intense migraine attacks.
What are situations that could allow me to stop migraine preventives?
Here are five situations where migraine can be drastically improved and preventive medications might be stopped:
- Retirement
- Menopause (especially in women with hormone-sensitive migraines)
- Resolution of a major personal stressor or conflict
- Successful management of a major medical issue (sleep apnea is a common example)
- Radical and sustained changes in your lifestyle
What is “the virtuous circle of migraine”?
Using migraine preventives can lead to a virtuous circle that may allow you to stop the drug. It’s easier to adopt a healthy, migraine-friendly lifestyle when one is feeling better and life becomes more predictable. Anxiety and depression may improve as you gain some control over your life. Migraine frequency may drop even further, and the preventive might be stopped.
Are there situations where the preventive will stop working?
That may happen. But before concluding that your preventive does not work, consider the following possibilities.
- Migraine tends to fluctuate spontaneously. Maybe this is just a bad phase.
- Is the deterioration caused by a factor that can be addressed, like a major change in stress levels or lifestyle?
- Is it possible that you have reset your normal? It is common that as people get better, they may feel that 6 days of migraine symptoms is bad. However, when they were having 12 days per month, 6 was actually quite good.
FAQ References
- Argyriou AA, Mantovani E, Mitsikostas DD, Vikelis M, Tamburin S. A systematic review with expert opinion on the role of gepants for the preventive and abortive treatment of migraine. Expert Rev Neurother. 2022;22(6):469-88.
- McGeeney BE. Cannabinoids and hallucinogens for headache. Headache. 2013;53(3):447-58.
- Nutraceuticals in Migraine: A Summary of Existing Guidelines for Use. Rajapakse T, Pringsheim T. Headache. 2016;56(4):808-16.
- Pringsheim T, Davenport W, Mackie G, Worthington I, Aube M, Christie SN, et al. Canadian Headache Society guideline for migraine prophylaxis. Can J Neurol Sci. 2012;39(2 Suppl 2):S1-59.
- Rajapakse T, Pringsheim T. Nutraceuticals in Migraine: A Summary of Existing Guidelines for Use. Headache. 2016;56(4):808-16.
- Tepper SJ. History and Review of anti-Calcitonin Gene-Related Peptide (CGRP) Therapies: From Translational Research to Treatment. Headache. 2018;58 Suppl 3:238-75.
- VanderPluym J, Evans RW, Starling AJ. Long-Term Use and Safety of Migraine Preventive Medications. Headache. 2016;56(8):1335-43.
More Resources on Acute Treatments

Supplements & Migraine
Supplements for Migraine Treatment, Prevention, & Management Supplements for Migraine Management can play a meaningful role in a holistic approach to preventing and managing migraine. In this...
New Canadian Migraine Treatment Guidelines
The Canadian Headache Society has released its New Canadian Migraine Treatment Guidelines, featuring the latest evidence-based recommendations to enhance migraine care. These updated Migraine...

Dosing of preventive treatments for Adult Migraine in Canada
The Adult Preventive Dosing Guide is your ultimate resource for understanding and choosing from the wide range of preventive migraine treatment options available in Canada. This comprehensive guide...

Preventive Medications to Reduce your Migraine Attacks
Are your migraine attacks becoming more frequent or severe? Is their impact disrupting your daily life? This resource explores the decision to start preventive migraine treatments, focusing on how...

Gepants for Preventive Treatment: Pills that Block the CGRP Receptor
Are you exploring your options for migraine prevention? Curious about gepants? Gepants are migraine-specific medications designed based on the scientific understanding of CGRP’s role in migraine...
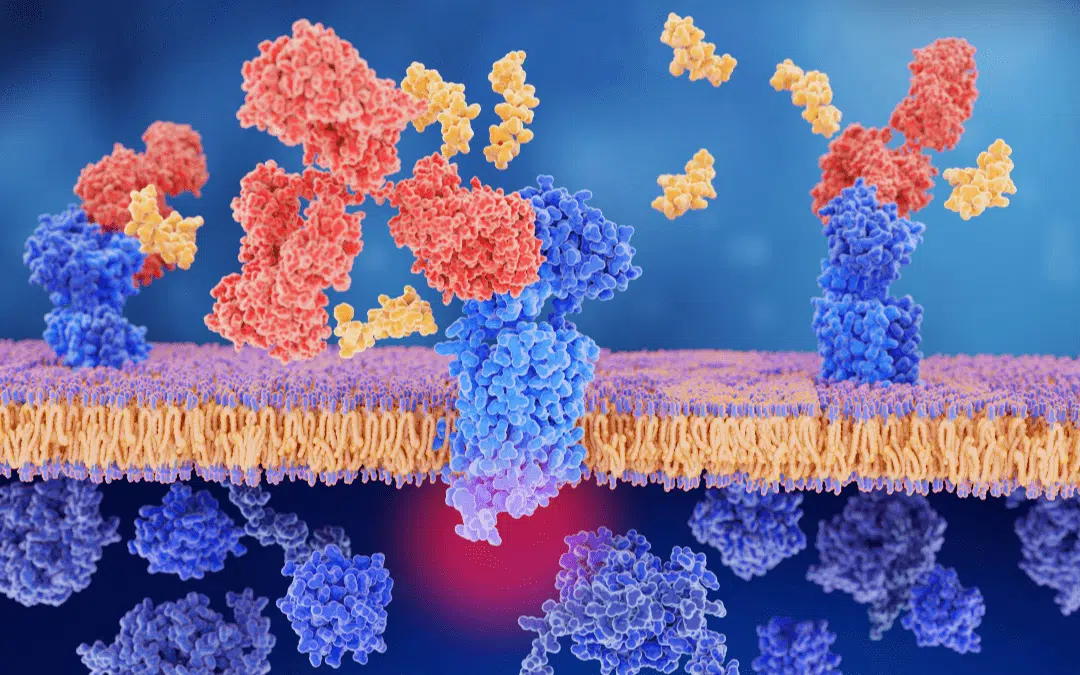
CGRP Monoclonal Antibodies: A Breakthrough Option for Migraine Prevention
Are you exploring your options for migraine prevention? Curious about CGRP monoclonal antibodies? CGRP antibodies are the first preventive medication developed specifically to treat migraine. This...
CGRP Monoclonal Antibodies (MABs): Summary and Effectiveness
Discover the latest advancements in migraine treatment with CGRP monoclonal antibodies. These innovative treatments target the calcitonin gene-related peptide (CGRP), a key player in migraine...

CGRP Monoclonal Antibodies (MABs): Risks and Side Effects
Understanding the risks and side effects of CGRP monoclonal antibodies (MABs) is crucial for those considering these treatments for migraine prevention. In this detailed overview, we discuss...

Vitamin D for Migraine Prevention
Many people with migraine seek non-medication strategies to help improve their condition. A recent study highlights Vitamin D as a promising supplement for migraine prevention. Discover how this...

Migraine Talks Episode 9: Preventive Treatments for Migraine
If you live with frequent or chronic migraine and are curious about preventive treatments but don't know where to start, this episode is for you. Dr. Elizabeth Leroux provides a clear summary of the...

How Food and Nutrition Can Impact Migraine
Curious about how food can impact your migraine? Food is often the first line of defense against migraine, but it’s important to remember there's no one-size-fits-all approach to diet. This...

Botox for Migraine: How Does It Work and How Effective Is It?
Curious about using Botox for migraine relief? Botox isn't just for cosmetic use—it's also approved to treat chronic migraine. This article delves into how Botox works, its effectiveness, and who...