Mandy, 27, has migraines since she’s 15. She has more migraines during her period. Her usual frequency is 10 days per month. She’s tall, lean, and has hyperextensible joints. She used to practice yoga and light weights, but now she’s working full time as a market analyst and she’s sitting most of the day. At night, she’s exhausted and watches TV. Since one year, she has developed neck pain, and more recently jaw pain. Her posture is slouching. Her migraines develop during the day. She tried amitriptyline but was too somnolent with it and stopped.
Neck pain can be caused by a bad posture and trigger migraines. Jaw pain can accompany neck pain.
STORYBOX 2:
Paul, 56, had very occasional migraines with aura. In fact, they were now happening a few times per year. Last year, Paul had a car accident with a whiplash. Since this even, he has chronic neck tensions and his migraine have reappeared, but now are starting with a deep pain on the right side of his neck. Sometimes he also feels a burning and some ice picks. An occipital nerve block provided him relief for a few weeks.
Neck pain can be caused by a trauma and trigger migraine. Occipital neuralgia can accompany other types of neck pain.
STORYBOX 3:
Tamara, 42, has chronic migraine. She rarely has a day without some headache. She never had head trauma. She exercises gently a few times per week with a program designed by a physio. Despite all this, when a migraine starts, she feels a lot of tension in her neck and down the shoulders. She tried a few preventives, with no success. Interestingly, after three treatments of Botox, her migraines are 70% better and the neck pain is gone.
Neck pain can be caused by migraine in a person with a normal neck and posture.
Anatomy Fact:
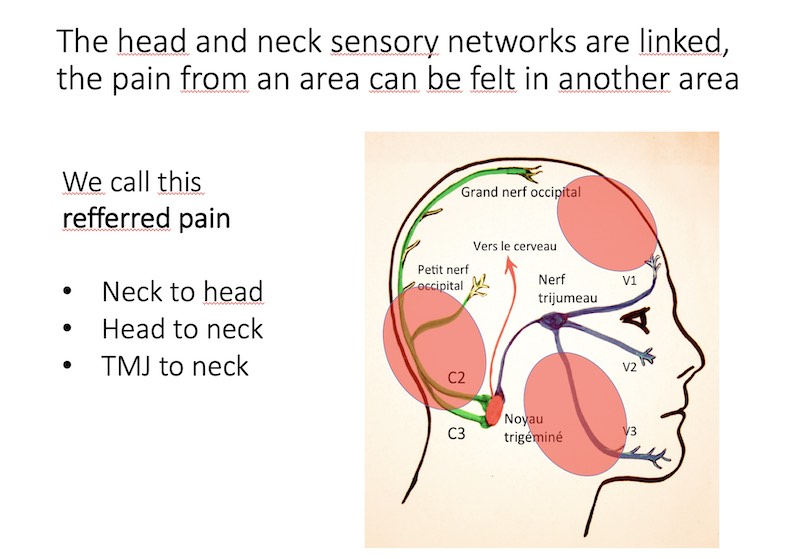
In humans, the head and the neck pain networks are linked and can cross-talk
The human anatomy explains why head pain and neck pain are often related.
The sensation of the face, head, sinuses, teeth, jaw are carried through the trigeminal nerve (V1, V2, V3). The trigeminal nerve also manages the sensations of the meninges inside the skull, where at least part of the migraine pain comes from.
The sensation of the neck and upper shoulder are carried through the cervical nerves (C2, C3, C4). Both networks connect in the same place (trigeminal nucleus), on the same neurons. Think of electric wires connecting on the same central box.
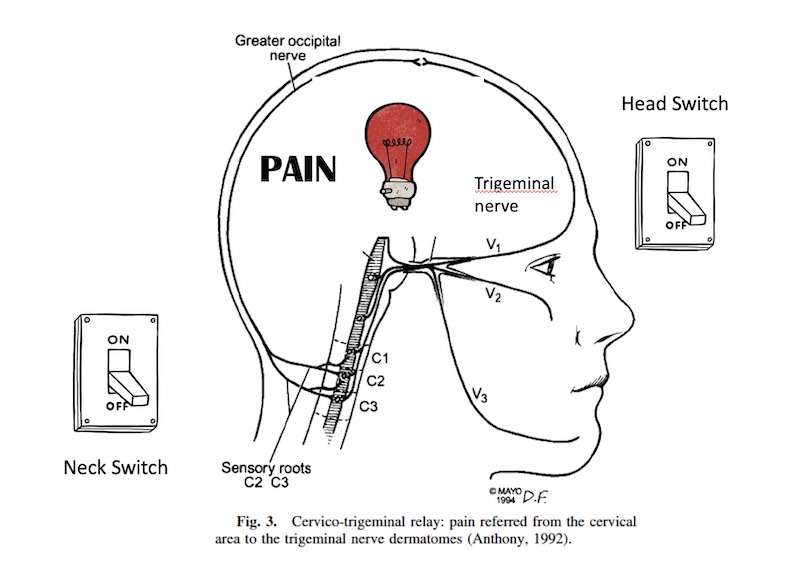
Another way to think about it is to imagine a light bulb connected to different switches. Neck switch? Pain network on. Meninges/migraine switch? Pain network activated.
What is cervicogenic headache?
In theory, cervicogenic headache is a headache that is caused by a problem in the neck. A cervical nerve block should provide significant relief as it treats «the cause» of the problem.
This definition does not address two very common situations: a person with migraine who has neck pain and a person who has post-traumatic headache with neck pain.
Migraine Ping Pong Theory, neck version:
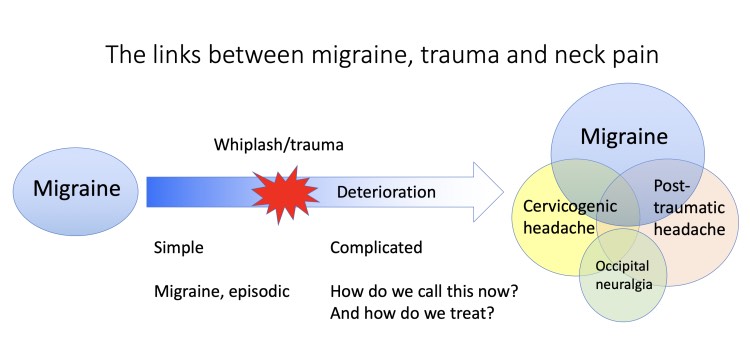
A neck problem can cause migraine, and a migraine can cause neck pain. Moreover, a bad migraine might trigger a contraction in the shoulder muscles, creating a vicious circle of pain. Severe migraines might also decrease the ability to exercise and contribute to deconditioning. In this situation, the neck is part of the problem, but not the «only cause». See more on the Ping Pong theory (See this post)
The complicated case of post-traumatic headache:
Traumas may cause persistent neck pain, and in fact, most cervicogenic headache research is done on people who have post-traumatic headache. This confusion in the classification is not helpful to patients and hopefully will be adapted in the future. Considering the fact that migraine is a risk factor for persistent symptoms after a trauma, you can get into a situation with multiple factors, and this situation is common in real life.
Occipital neuralgia: what is it?
A neuralgia is a pain caused by a problem in a specific nerve. Usually the pain is electrical, there is a sensory deficit (tingling, numbness) in a clear skin territory and blocking the nerve relieves the pain. As many migraine people have allodynia (skin sensitivity), pressing on the occiput will cause pain, but that does not mean that a nerve is really compressed. Many clinicians wrongfully diagnose occipital neuralgia in migraine patients.
How does the physician diagnose cervicogenic headache?
There is no unique answer to this question, as there is still a lot of controversy about this. In theory, Cervicogenic headache excludes people with migraine and trauma. Also in theory, cervicogenic headache should be diagnosed based on some «proof» like imaging, examination etc but in real life we do not have reliable tests to diagnose cervicogenic headache.
One technique used as a diagnostic test is to do a C2-C3 blockade and see if the headache gets better, proving the origin of the problem. But this technique is not perfect. It can lead to a placebo response or to a failure in refractory situation still caused by a neck issue.
What can be done to treat cervicogenic headache?
Usually, a global approach including physiotherapy (strengthening and stretching), medications, blocks and other techniques to manage chronic pain is adopted. Many patients consult chiropractors and osteopaths for this problem. The chiropractic and osteopathic theories should be discussed separately as they are controversial from the point of view of traditional medicine. Cervicogenic headache is usually not an easy situation and it may require long term management.
REFERENCES
Bogduk N, Govind J. Cervicogenic headache: an assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurol. 2009;8(10):959-68.





{kind=link}